
Frontiers Friday #127: Dropout (Part I)⭕️
A distillation of key strategies to reduce premature termination from psychotherapy.
Let's kick-off this series on dropouts in psychotherapy treatment with some definitions. For the purposes of our discussion, dropout does not mean people who make an unplanned ending after they've experienced positive gains from treatment. Most recent research study would use the working definition on dropout as
People who discontinue unilaterally without experiencing reliable improvement.
What are the rates of dropouts in psychotherapy? About 1 in 5 clients dropout. But, as stated in our book Better Results, "there's a huge variance between studies ranging from of 5% to 70%! Dropout rates are typically higher in child and adolescent population (40-60%)."
Don’t brush off this topic on early termination lightly, even though at first blush, the reasons for a client dropping out of treatment might seem fairly obvious (e.g., client not engaged, lack of motivation, not experiencing any benefit).
From the treatment provider perspective, experiences of client dropping out of therapy can be demoralising. Yes, at times we knee-jerk to putting the onus on clients, but for the most part, therapists feel responsible and experience disappointment, confusion and shame.
If we take the time to examine carefully, we just might be able to pre-empt potential disengagement, address any therapeutic ruptures, and make room to help our clients speak the unspokens with us.
A sidenote about this week’s Frontiers Friday: After typing out today’s piece, I’ve decided that, instead of the usual five curation, I’ve decided that for today, I’d focus on one, coupled by an exercise you can do (see at the end of this post). This is because the recommendations from this excellent book are highly valuable. Plus, I do not want to overload you.1
Here we go.
📕Must-Read: Premature Termination in Psychotherapy: Strategies for Engaging Clients and Improving Outcomes

This 2015 book by Joshua Swift and Roger Greenberg is one of the best resource on this specific topic. The researchers have drawn from a large body of work.
(Also, we are thrilled to have Joshua Swift contribute a chapter in our upcoming book, The Field Guide to Better Results.)
I recommend that you read the book. For now, here’s my summary.
Key Grafs:
(note: I’ve added some of my perspectives next to the key highlights from this book when it’s relevant. I’ve labeled them as ‘DC.’)
A. Occurrences:
- About 1 in 5 people terminate treatment prematurely.
- Specifically, “The average dropout rate across all studies was only 19.7%, with a 95% confidence interval of 18.7% to 20.7%.” (p. 171).
- University-based clinics, including psychology department training clinics and university counseling centers, experienced the highest average rates of premature discontinuation. This is likely due to younger clients, trainees providing the services, lack of investment and perceived credibility due to nil or minimal fees charged.
B. Strategies:
- Frequency expectation: The mere act of specifying duration was associated with lower dropout rates.
- Most people expect to attend only a few appointments, but if made aware that a greater number of sessions are involved, “they know what to expect and are more likely to follow through with that expectation.” (p. 49). (DC: Though I do not provide an exact number, I usually say to my clients that we’d meet for just a few sessions to see if this is helpful. Plus, I’d monitor their progress using outcomes measures session-by-session. If things aren’t going in the right direction, it’s my responsibility to tweak/adjust/calibrate in order to better help them. Finally, it’s my job to render myself out of a job.)
- Provide role induction: i. what to expect (process, treatment rationale), ii. role of therapist, and iii. role of client. (DC: As I’ve outlined in the Structure and Impact Course, I talk about the need to provide a scaffold based on figuring out“Where are we, where we are going, and why.”)
- (DC: Do not take for granted what client might expect from therapy. I recall a particular case where the client thought that therapy was supposed to “happen” to him, just like in the movies where he laid down on a couch while I analyse him behind his back.)
- Don’t forget to address logistical concerns. (DC: This could relate to issues with transportation, finances, caregiving responsibilities, etc. We can also use systems to help people with their logistics. For instance, in our group practice, we found that simply having an automated sms reminder 48hrs prior to their appointment dramatically reduced DNAs. The unintended consequence of this was that in some rare occasions, clients arrived at the right time, but one day earlier!).
- The curvilinear relationship between outcome expectation and treatment dropout:
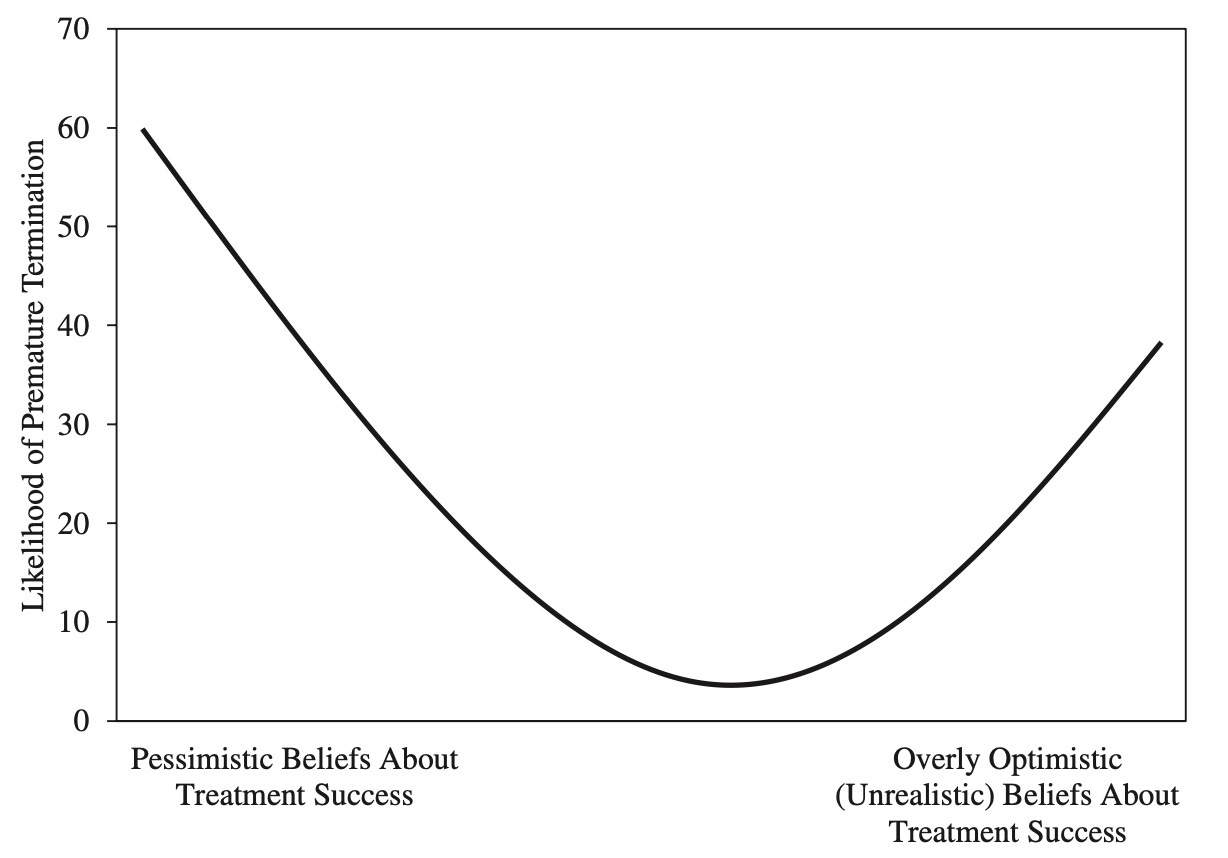
- “Not only is it important for clients to believe that the treatment will help, they should also believe in the effectiveness of their therapists.” (p. 119). (DC: This speaks to the importance of a therapists needing to do something that they themselves believe in).
- Distinction between client expectation and client preferences: “preferences represent desires and values, expectations reflect what clients actually believe should or will happen in therapy.” (p. 80). (DC: I would argue that it would do everyone good to match unique preferences at the pre-therapy phase, if there’s any. For instance, someone has a specific preferences of seeing a female, someone with a particular spiritual orientation, etc.)
- “…clients who receive their preferred conditions were between one half and one third less likely to drop out of therapy prematurely compared with clients who did not receive their preferred therapy conditions.” (p.85)
- Planned Termination can lead to lower rates of premature discontinuation. (p.98) (DC: I’ve observed this in our Supershrinks study as well. More effective therapists have a higher rate of planned endings. On a practical note, at the start or even pre-therapy phase, I would recommend enquiring about clients initial thoughts of expectations on treatment length).
- Address the fact that focus of therapy may change over time, thus treatment length might change.
- Address issues regarding a decline in hope or motivation.
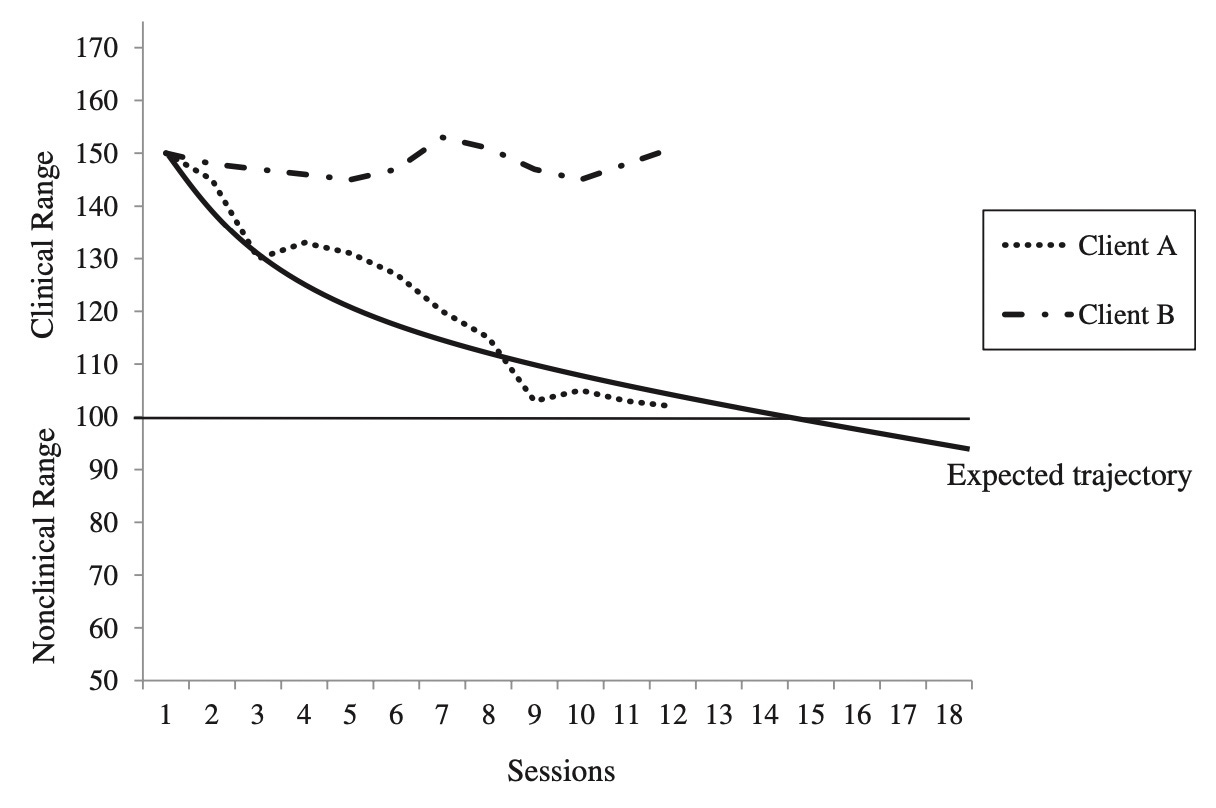
- Therapists are poor judgers of recognising when their clients are getting worse.
- Monitor progress systematically, because a client is more likely to dropout if it deviates from expected trajectory (see figure below).
Reflection: Contemplative Action and Active Contemplation
The following is an area of deliberate practice that are underrated by many clinicians. It’s not fanciful, and frankly, quite tedious at first.
A. Contemplative Action:
Park aside some time next week or so to look through your caseload.
i. Who are the ones who terminated therapy prematurely in the face of lack of improvement?
ii. What are your baseline rates of dropout?
iii. For each case, how do you decide if there was improvement or not?
iv. Do you have a system to zoom out and look at all of your past cases?
B. Active Contemplation
i. Solve not just for specifics, but solve for patterns. What can you learn about the people who dropped out from treatment prematurely?
ii. What can you learn about you?
iii. Tax the system before taxing the human. What are some systems in place to help you not only keep track of people who might fall off your radar, but also help you prevent unnecessary dropouts from treatment?
BIG HUGS TO NEW PEOPLE WHO ARE AT THEIR FRONTIER!
If you've just joined us, I'm glad you can join us at the "bleeding edge." Feel free to check out the back catalogue of Frontiers of Psychotherapists Development (FPD). You might also want to go into specific topics in the FPD Archives like
And if you want to see past newsletters, the entire archive is now made available in substack.
See the most recent missives by topics:
Devotion to the Craft (6 Parts)
Caring for People in Organisations (3 Parts)
Clinical Supervision (3 Parts)
Feedback Informed Treatment (4 Parts)
Unintended Consequences (2 Parts)
Deep Learner (4 Parts)
Going Further with Deep Learner and The Use of Obsidian (6 Parts)
See What You Hear, Hear What You See (4 Parts)
Trauma (3 Parts)
Deliberate Practice (5 Parts)
Empathy (6 Parts)
Therapist Effects (2 Parts)
Client Point of View (4 Parts)
Tech Tools for Therapists (4 Parts)
Emotions (6 Parts)
Sensitivity (3 Parts)
Alliance (6 Parts)
Existence (6 Parts)
Play (4 Parts)
Humour (4 Parts)
For the general public, my other blog site is called FullCircles: Reflections on Living
By the way, don't feel bad if you want to unsubscribe to this newsletter. This might not be for you. The last thing I want is to add to the anxious clutter in our inboxes. And, please excuse any typos…
Note:
These newsletter are free, but many hours are spent handpicking the curated list… as well as writing the essays and recording the videos and podcasts that make it to Frontiers Friday . Amazon affiliate links, if any, are to help ease the costs. You can also support the sustenance of this work by picking up any of the books, dive deep into our courses, or gifting them to others.
Update: Substack has added a “PLEDGE” somewhere on the page. Thanks for those who are so kind to want to support my writings. I do not have a paid subscription option to Substack at this stage. Still, if you pledge, it means a great to me. Big thanks.

Daryl Chow Ph.D. is the author of The First Kiss, co-author of Better Results, and The Write to Recovery, Creating Impact, and the forthcoming book The Field Guide to Better Results .
The Field Guide to Better Results is coming out soon on 23rd of May’23!
I have gotten some comments that while they value the resources from Frontiers Friday, they can’t keep up!