
The Negative Effects of Psychotherapy (Part I. #225) ⭕️
This could happen to you.

This couldn’t happen to you, could it?
Chances are, this might have even happened in your caseload without you realising it.
Most therapists are aware that clients may have negative experiences, but how often does this actually happen?
Adverse events are expected to impact more than 1 in 10 clients undergoing psychotherapy.
While most clinical research tends to focus on the positive effects of psychotherapy, according to researchers Jenny Rosendahl and colleagues, there has been a rapid increase over the last decade publishing the negative effects of treatment.
However, on a clinical practice level, the nuanced conversation about different kinds of adverse effects of therapy is rarely discussed among practitioners and clinical supervisors.

In their recent review article titled, “Contextualising the Negative Effects of Psychotherapy,” Rosendahl and team did a tour de force of the existing evidence looking at the adverse outcomes caused by the endeavour of therapy.
To start off, the authors made a useful conceptual distinction between terminologies used in the clinical literature:
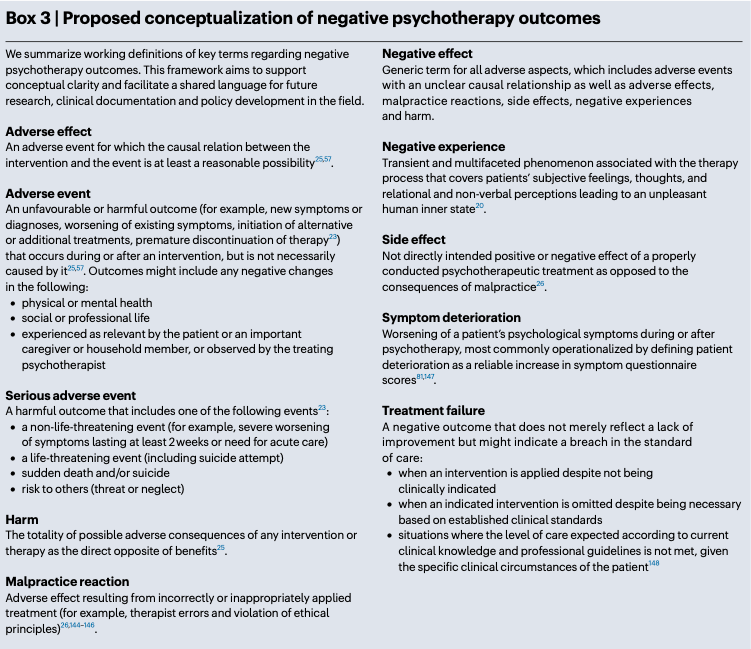
Let’s zoom in on three of the terms:
1. Side-Effects of Therapy:
This term describes a negative outcome of a properly conducted psychotherapeutic treatment. It is specifically differentiated from consequences that arise from malpractice.
Side effects are not necessarily negative, but refer to effects not directly intended. For example, emotional distress during exposure therapy might be a transient and even intended side effect to facilitate progress.
2. Harm
This refers to “the totality of possible adverse consequences of any intervention or therapy, serving as the direct opposite of benefits.”
3. Adverse Event
This is defined as any negative change in physical or mental health and/or in social or professional life, experienced as relevant by the client or caregiver.
It is an unfavourable or harmful incident that occurs during or after an intervention but is not necessarily caused by it.
Examples include new symptoms, worsening of existing symptoms, initiation of alternative treatments, or premature discontinuation of treatment.
Slippy Slope
Needless to say, malpractice and unethical behavioural fit this category of negative outcomes.
Take a look a closer look at the summary table above.
The researchers noted that sexual misconduct, which has been dubbed the Slippery Slope, occurs up to 9.4% with male psychotherapists and up to 2.5% with female psychotherapists.
Though the percentages look relatively low, it still strikes me as shockingly high.
Patients’ Perspective
The authors categorised five different categories of negative experiences and adverse effects of psychotherapy from patients’ perspectives.
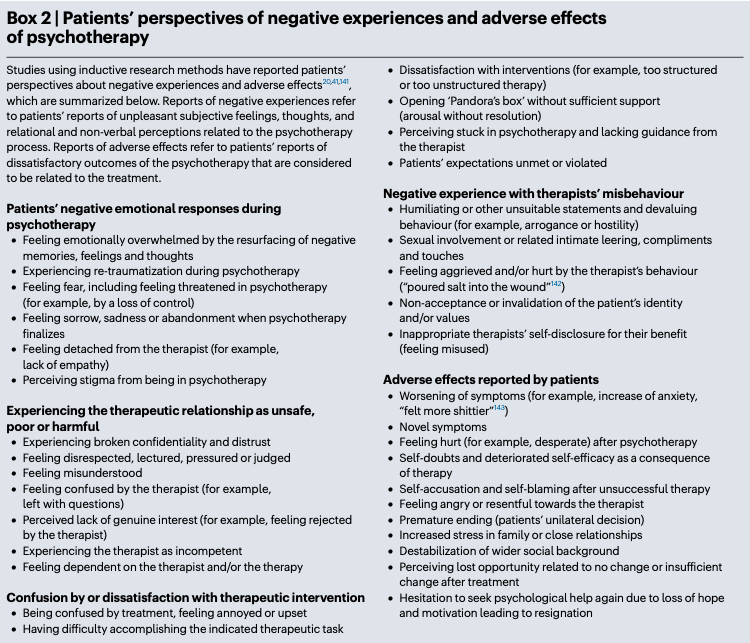
My suspicion is that we don’t hear so much of this happening in our caseload, but we hear about them from our new clients.
They tell you about their past experience with a therapist who made them feel invalidated, feeling a lose of hope after a treatment failure with their 5th therapist, feeling confused and annoyed by the passivity of their past psychologist.
RELATED:
See specific client’s stories of being let down.
Negative Effects in Children and Adolescent Population
Rosendahl et al. point out that the negative effects with youths should be specifically studied.
They note three reasons:
Limited influence and power of the child.
Heightened vulnerability during formative period of development.
Because treatment with a child involves caregivers, this may impact the integrity and autonomy of both the child and other family members.1
Both studies in the adult and youth population is clear. Deterioration can happen due to treatment failure.
What are the rates of deterioration?
About 6 to 8 percent.
In other words, for every 12-17 clients that you see, one of them are likely to get worse under your care.
The question is, do we know when this is happening in real-time?
Differences in Public and Private Setting
Is there a difference depending on the context of treatment?
The article noted that in community mental health settings (treatment delivered through a coordinated, comprehensive services model mainly to lower-income youths facing severe stressors), 19% of the young patients showed symptom deterioration.
In private managed care settings (mainly individual psychotherapy delivered by a single mental health professional to usually well-resourced youth), 13% of young patients showed symptom deterioration.
Recommendations
Finally, this paper spells out several recommendation for training, clinical practice and research.
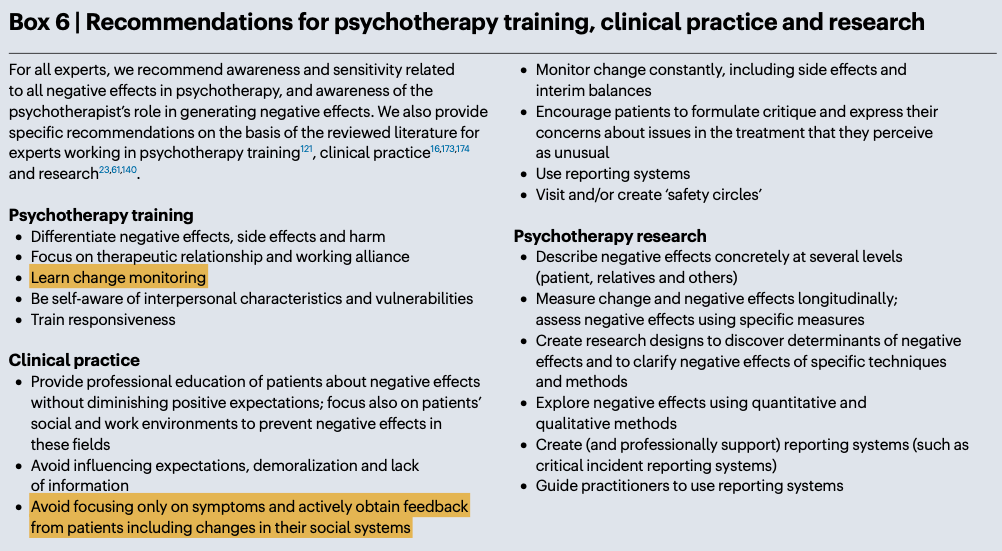
For the purposes of most readers here on Frontiers of Psychotherapist Development (FPD), I’m going to focus on training and clinical practice.
There are two worth highlighting:
1. Learn Change Monitoring
What the researchers mean by this is to equip therapists in training with the skills and knowledge to systemically track and assess a client’s progress through the course of treatment.
Having a pre-post measure does not constitute this. Measuring outcomes at the beginning, middle and end is a form of evaluation, rather than adaptation.
Adaptation means, to let your client’s dataset change your mindset.
In feedback-informed treatment (FIT), we talk about the importance of being sensitised to change that occurs between sessions and to utilise them.
SEE RELATED:

2. Avoid focusing only on symptoms and actively obtain feedback from patients including changes in their social systems.
I didn’t expect this to be in their recommendations for clinical practice.
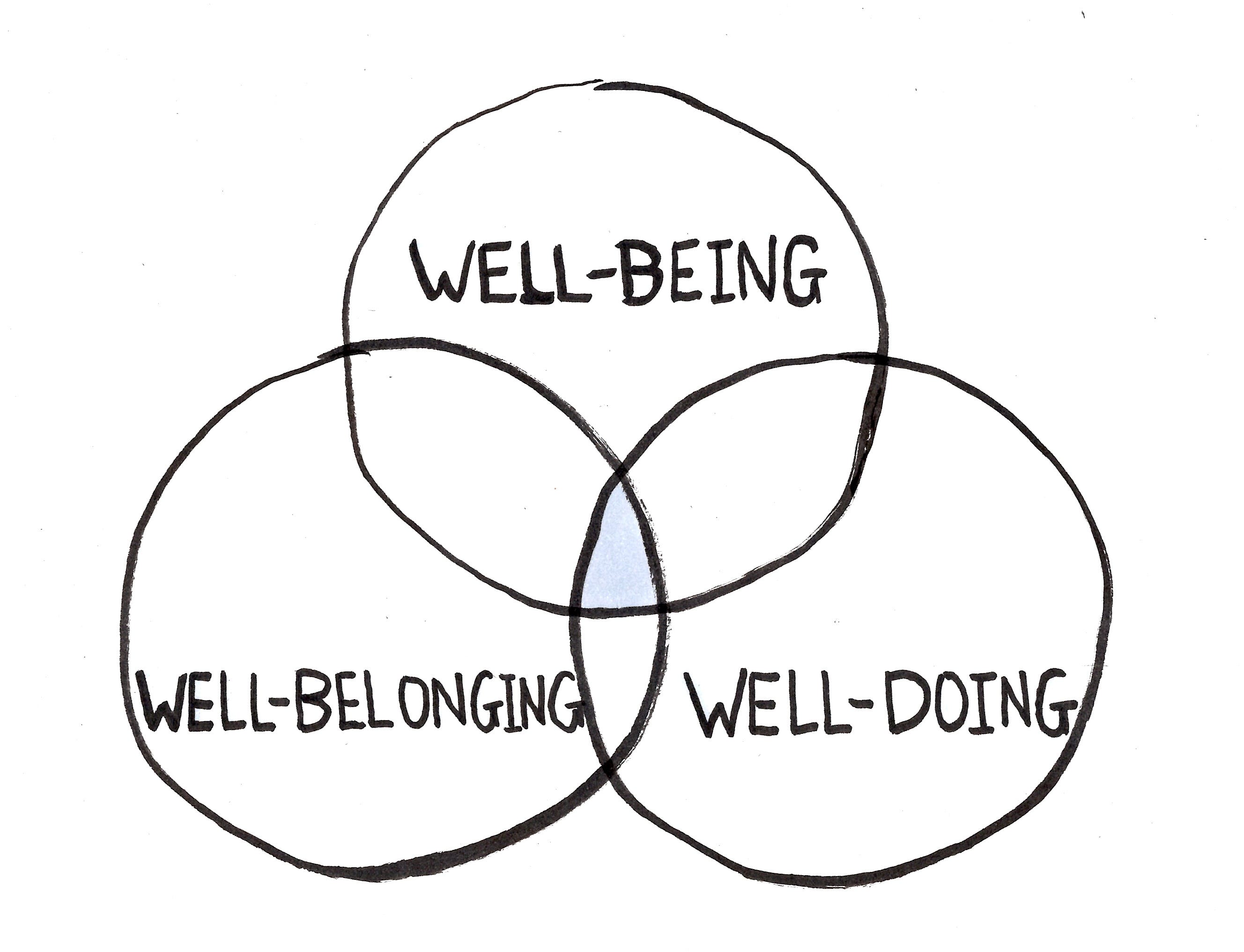
In trainings and consultations, I suggest to therapists to measure what matters most to clients, which is often not just about their symptoms, but their experience of life, which pertains to their well-being (how they feel on the inside), well-belonging (their relationships with people they care about), and their well-doing (work, occupation, daily meaningful activities).
This particularly hit home for me when I was working in a psychiatric setting, specifically with an early psychosis intervention team. I saw situations when symptoms of voice hearing stayed the same, but their relationships were improving. Conversely, I saw clients who had a reduction in positive and negative symptoms of psychosis, but their global wellbeing measures didn’t improve.
However, on the point of focusing solely on symptoms, Rosendahl and team highlighted the flip side that I hadn’t fully considered.
• Broader Impact of Psychotherapy: Unlike pharmacological treatments, psychotherapy's effects extend beyond just clinical symptoms to influence a client’s social and emotional functioning. This broader impact means that negative outcomes can manifest in various aspects of a patient's life.
• Wider Spectrum of Negative Outcomes: Negative effects can include changes in physical or mental health, but also in social or professional life. For instance, increased self-esteem might lead to conflicts at work, resulting in "moderate" negative effects such as strained professional relationships or job loss.
• Subjective Meaning and Life Impact: The assessment of negative effects should consider not just immediate symptom changes, but also the evolving subjective meaning and broader life impact. A patient's emotional or behavioural changes during therapy could, for instance, lead to changes in family relationships that are experienced as undesirable by relatives, even if the patient experiences them differently.
Likewise, when psychotherapy is at its best, it has a good generalisation effect. If we only measure symptoms, we miss the messy richness of what it a good life ultimately constitutes. Not just an absence of symptoms, but a full engagement of relationships and doing things that bring meaning.
If we don’t measure at all, we become less sensitised to ebb-and-flow and changes from session to session.
Beyond measuring outcomes, there is also the alliance piece. Measuring the alliance at each session helps you catch instances when the session may have been a little off-track for the client.
Open Up to Conversation and Learning
This is an important conversation to have between colleagues and in the field at large.
I don’t think we do a good job of learning from our mistakes.
Part of the reason is because of survivorship bias. We don’t know when a negative outcome occurs because our clients don't turn up for their next appointment.
The other reason is because most therapists don’t systemically keep track.
Here’s what you can do:
Learn to employ a feedback informed approach to your clinical practice.
Keep track of your mistakes.
Share them amongst your colleagues.
The practice of psychotherapy should not be a lone sport.
Learn from the mistakes of others. You can’t live long enough to make them all yourself.
— Eleanor Roosevelt
If this is worth reading, please share this with one of your colleagues.
P/S: Hat tip to the co-author Zbyněk Vybíral for sending me the paper.
Notice Board:
Our 3rd Cohort for the Deliberate Practice (DP) Cafe is about the kick-off in Nov 2025. If you are keen to join Scott Miller and I, and a small group of like-minded practitioners from all over, join us! Only 4 more seats left.
Register now.

Daryl Chow Ph.D. is the author of The First Kiss, co-author of Better Results, The Write to Recovery, Creating Impact, and the latest book The Field Guide to Better Results. Plus, the new book, Crossing Between Worlds.

You might be interested in my other Substack, Full Circles: Field Notes on the Inner and Outer Life.

It can also be true when there is a lack of involvement with parents of the young person.
Yes, the negative effects of therapy does happen to about 1 in 10 of my clients, according to my Feedback Informed Treatment (FIT) data. Daryl, thanks for breaking down the data from Jenny Rosendahl and her colleagues citing the increased number of publications in the last decade on the negative effects of psychotherapy.
As you say: “If we don’t measure at all, we become less sensitised to ebb-and-flow and changes from session to session.
Beyond measuring outcomes, there is also the alliance piece. Measuring the alliance at each session helps you catch instances when the session may have been a little off-track for the client.
…Here’s what you can do:
1. Learn to employ a feedback informed approach to your clinical practice.
2. Keep track of your mistakes.
3. Share them amongst your colleagues.
The practice of psychotherapy should not be a lone sport.”
I just stumbled upon your well-structured article on the negative effects of psychotherapy. Two weeks ago, I published my take on the subject. I think you might like it: https://thehumanconditionrevisited.substack.com/p/mostly-harmless-understanding-and