
Frontiers Friday #104. Alliance (Part I) ⭕️
Handpicked Recommendations and Highly Relevant Research on Working Alliance

As a child, my uncle used to perform magic tricks for my cousins and I. What a thrill to see things disappear out of thin air and reappear behind our ears. He was a really good entertainer (He's a master puppeteer now). Later in life, I learned a bit about magic. I had a friend in school who became a close-up magician (I wrote about this here). But the thing is, as the great magician Jamy Ian Swiss noted, it’s easy to figure out how a trick is done, but the real difficult part is to develop the art of doing it.
What has this got to do with psychotherapy?
Knowing about how the therapeutic alliance works is quite different from how it's done in the conversational reality and healing space of therapy.
In the late 1930s, a young psychologist noted the following:
“… A full knowledge of psychiatric and psychological information, with a brilliant intellect capable of applying this knowledge, is of itself no guarantee of therapeutic skill.
The essential qualifications of the psychotherapist lie primarily…the realm of attitudes, emotions, and insight, rather than in the realm of intellectual equipment.”
This was none other than Carl Rogers.1
As you plunge in to this topic of Working Alliance in the coming weeks of Frontiers Friday, I urge you to do the following:
Write down what you currently know about therapeutic alliance (alliance predicts outcomes, etc.). Elaborate as much as you can,
Read each of the recommendations made, or at least the summaries I provide in this series, and finally,
Note down how does the new input connect with your prior knowledge2.
As we talk about this in the online course Deep Learner, our mind is a prediction machine, seeking to be confirm or disconfirmed by new inputs, so as to update our internal models, and then better adapt to the external world.
While some of the research findings discussed in this post and upcoming ones might fit with your intuition, others might be more naunced and might counter what you originally thought. It’s really easy to feel like “you-knew-it-all-along.” I must admit, I did when I was going revisiting some of the research. But there was a time when I didn’t know some of the stuff that I’m about to share with you. It just feels as if I knew it all along.
The key is to be able to connect with the new inputs with your prior knowledge and make new and relevant insights.
That's the magic of learning.
Special Note:
You may have noticed that Frontiers Friday looks different. After much deliberation, I've bit the bullet and switched platforms. I hope to write more about this and why I've made the decision. This will likely be under an essay I’m writing about regarding business models practitioners find themselves under, be it as an employee, business owner or a contractor, and why we need to think clearly about this.
Tell me what you think in the comments (yep, that’s one of the new features in our newsletters), and help spread the word.
Big thanks.
📽 New Video from Frontiers, Therapy Tip of The Week: Embodied Cognition

It's easy to get lost in our heads. Our pet theories end up dominating and preventing us from being in touch with the person in front of us.
In Part 3 Therapy Tip of the Week, I'd talk about how psychotherapists can employ the principles of embodied cognition—the idea of embodiment as a way of thinking—to help you deepen your empathic understanding of your clients, especially in stuck situations.✍️From the Frontiers Archives: What Therapy Is (Or Isn’t).
The psychodynamic camp says, “Your past is the problem.”
The third wave mindfulness therapist says “Mindlessness is the problem.”
The emotion-focused therapist says, “Your unresolved feelings are the problem.”The pioneering team at Mental Research Institute (MRI), Palo Alto says “the attempted solution is the problem.”
The solution-oriented practitioner says “There are exceptions to the problem.”Pre-deciding what the problem is, is the problem. And just maybe, focusing on the engagement with each person is the way.
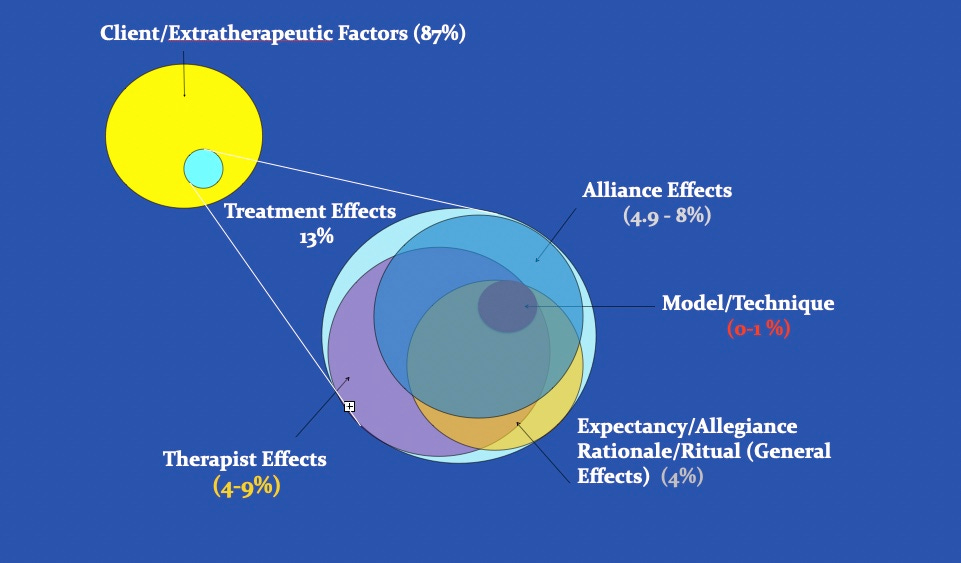
👀 Visual: How Much Does Alliance Contribute to Treatment Outcomes?
To put into perspective, how much does alliance contribute to outcomes, relative to other factors?
The answer: Based on a wealth of studies published over the last four decades, therapeutic relationship exerts about 5-8%, whereas models and techniques contributes about 1%.
📜 Research: It's Not Just High Alliance
In one of the largest study (2990 youths treated by 98 therapists) on the role of alliance in the treatment of adolescents--even larger than the number of all the samples combined in a meta-analysis (McLeod, 2011)--my colleagues and I found that alliance ratings that improve over time is more predictive of outcomes than alliance at a given point in time (i.e., mono-assessment model), or an aggregation of multiple alliance points (i.e., aggregate-assessment model), which most alliance-outcome studies tend to utilise.As counter-intuitive as it seems, lower initial alliance ratings that improves over time (i.e., low to high) is more predictive of good outcomes than high alliance ratings over time (i.e., high to high). Large changes in scores (from low to high) on the SRS across sessions accounted for 10% of the variance in outcomes compared with 1% for alliance scores that started either high or low but remained stable
Implication: Learning to elicit nuanced feedback early on is key.
(Also Available on ResearchGate)
⏸ Words Worth Contemplating:
”We've lost the 'care' in healthcare."~ Ai-jen Poo, author of The Age of Dignity.

Reflection:
How do we preserve the dignity of care in our work?
As a point of reflection, what do I need to do with my relationship with time, so that I am less hurried in my conversations?
As the late writer and poet John O'Donohue pointed out, stress is our perverted relationship with time.
BIG HUGS TO NEW PEOPLE WHO ARE AT THEIR FRONTIER!
If you've just joined us, I'm glad you can join us at the "bleeding edge." Feel free to check out the back catalogue of Frontiers of Psychotherapists Development (FPD). You might also want to go into specific topics in the FPD Archives like
And if you want to see past newsletters, click here.
In case you missed it, see the most recent missives
Caring for People in Organisations (3 Parts)
Clinical Supervision (3 Parts)
Feedback Informed Treatment (4 Parts)
Unintended Consequences (2 Parts)
Deep Learner (4 Parts)
Going Further with Deep Learner and The Use of Obsidian (6 Parts)
See What You Hear, Hear What You See (4 Parts)
Trauma (3 Parts)
Deliberate Practice (5 Parts)
Empathy (6 Parts)
Therapist Effects (2 Parts)
On Grief (4 Parts)
Client Point of View (4 Parts)
Tech Tools for Therapists (4 Parts)
Emotions (6 Parts)
My other blog site is called FullCircles: Reflections on Living
By the way, don't feel bad if you want to unsubscribe to this newsletter. This might not be for you. The last thing I want is to add to the anxious clutter of our inboxes.

Daryl Chow Ph.D. is the author of The First Kiss, co-author of Better Results, and The Write to Recovery, and the forthcoming books, Creating Impact,The Field Guide to Better Results
Note: These newsletter are free, many hours are spent handpicking the curated list that make it to Frontiers Friday. Amazon affiliate links, if any, are to help ease the cost of these missives.
P/s: Please excuse any typos!
Carl Rogers, 1939, p. 284 The Clinical Treatment of the Problem Child.
Educational psychologist David Ausubel said, ‘If I had to reduce all of educational psychology to just one principle, I would say this “ The most important single factor influencing learning is what the learner already knows. Ascertain this and teach him accordingly.”’