
DP for This, DP for That (Frontiers Friday #231) ⭕️
What we can learn from chubby thighs.

Note: A version of this was originally published on my blog in Nov 2025. I thought it would be good to share it on Substack. There are additional anecdotes and editing. I’m keeping future writings here instead.
You may have noticed a surge in books about deliberate practice (DP) in psychotherapy.
There is DP for CBT, DP for EFT, DP for DBT, DP for IPT, DP for MI…
The list goes on.
As one of my colleagues observed, there seems to more books on DP than published research papers on it.
I have nothing against any model-specific approaches. Personally, I gravitated to systemic thinking and experiential-based approaches. More recently, I revisited more on depth psychology.
Specific approaches offer specific metaphors. Metaphors represent and point to realities. They are fingers pointing to the moon; they are not the moon.
However, I’m not so sure that it makes sense to think about deliberate practice (DP) for specific schools of therapy. Back in Jan 2018, I said that this is one of the things to avoid in DP.
To my co-authors and I, working on a pre-ordained approach sounds more like purposeful practice (PP).
PP is more about narrow competence.
DP is more about personal excellence.
RELATED:

Learning from our past
There is a place for PP. There is a place to learn specific modalities as a starting point, not as an endpoint.1
However, our field has been peddling assumptions of specific approaches for specific issues for the last 60 years—and it hasn’t gotten us very far.
The cumulative evidence suggests that narrowing our horizons to specific dogma has made minimal advancement in enhancing effectiveness Not only that differences between models account for 0-1% of client outcomes,2 competency in specific modalities and adhering to specific protocols contribute next to nothing towards those we are trying to help.3
When I think back of various workshops on specific schools of thought that I’ve attended, be it in ACT, CBT, EFT, EMDR, Schema therapy, most trainers tell me to stick to the technique, so that I can get better at it.
The consequence of this communicates more of compliance than following my curiosity, and of what is cogent to me.
The Allure
Purposeful practice is appealing, both for clinicians and educators. Why? For two reasons. PP provides
Structure, and
Scalability.
First, the affordance of structure in specific models provides a clear pathway on what to work on, how to get better at it, and even a list of exercises you can do to get good at it, based on the assigned objectives and competency grading given.
Second, you can rinse and repeat. This “structure” allows more therapists to learn this at scale.
We tend to conflate structure with models.
New therapists inadvertently seek structure by learning a specific approach. This is limiting. We have to learn how to structure our sessions beyond specific modalities.
By zooming in prematurely and sticking to a specific model, you end up rigid in your method, coupled with a lack of grounding principles to guide you. (I’ve talked about the importance of structure elsewhere).
In terms of scalability of DP, there is no straightforward ‘factory’ solution because, as you might recall from previous issues, DP is highly individualised (compared the top of both pyramids).
It’s a hard, long road. No easy cookie-cutter solutions.
What you need to work on might differ from what I need to work on.
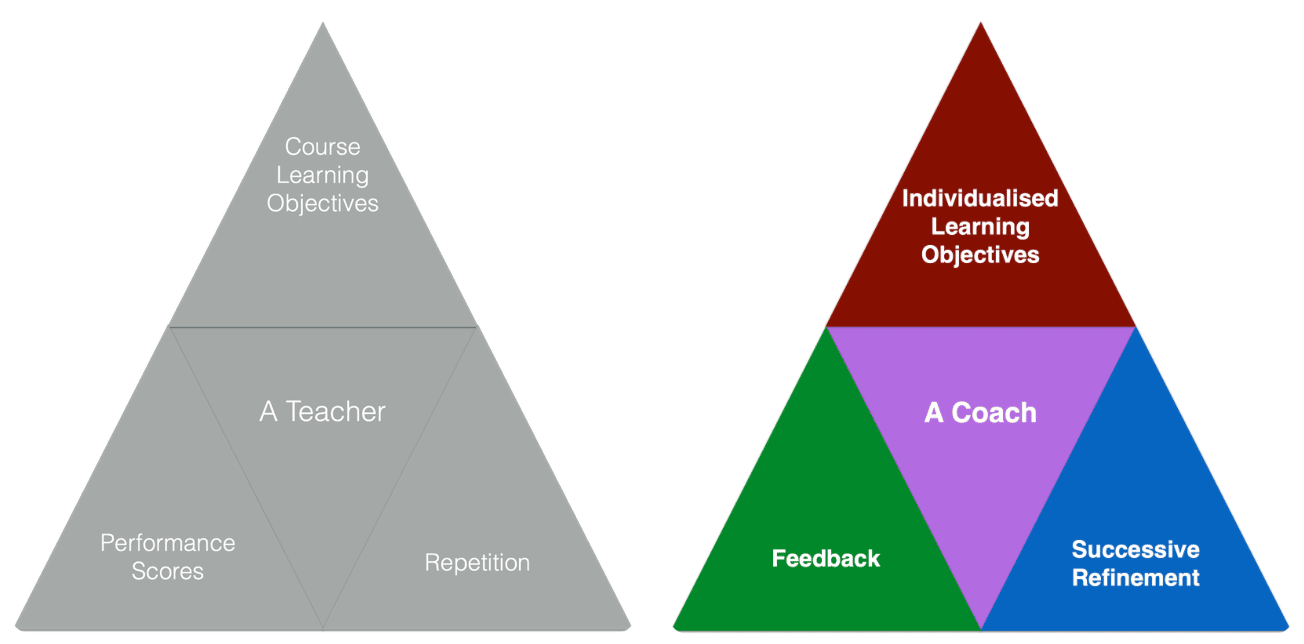
If you jump too quickly into ‘practice exercises’ without first figuring out if this is the right thing for you to work on (i.e., course learning objectives vs. individualised learning objectives), you could end up expending energy without actually translating to specific improvements (i.e., repetition vs. successive refinement).
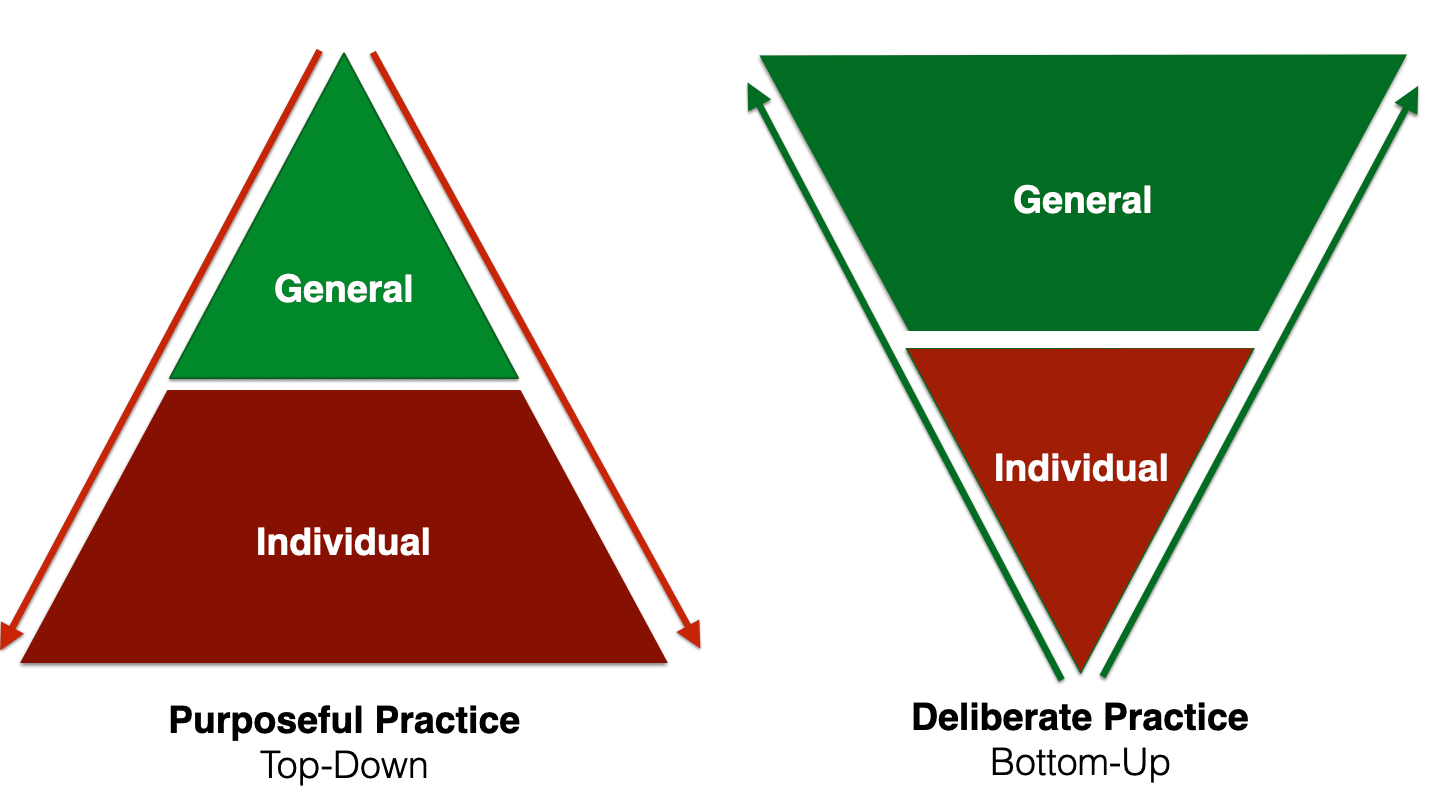
Another way of thinking about the difference between PP and DP is its general pedagogy. The method of teaching in PP is predominantly top-down (i.e., what you should learn), whereas in DP, the emphasis is more bottom-up (i.e., figuring out where each therapist’s existing ability is, tapping into their native wisdom and going from there).
Before we go further, here is an overview table for comparison:
Table Comparing Purposeful Practice and Deliberate Practice.

By analogy, if you were a musician, it’s much easier to practice scales on a piano than to get good at song craft. With scales, the target is well-defined. You keep working at it and you’ll get the result. With writing better songs, it’s less well-defined, it’s subjective, but you can work at it.
You might not even be technically proficient and still improve at song-craft.
Think of The Beatles. None of the fab four were technically proficient, nor did they even seem to know what chords they were playing at times.

In therapy, it’s much easier to work at thought challenging than it is to help a client have an impactful experience in the session.
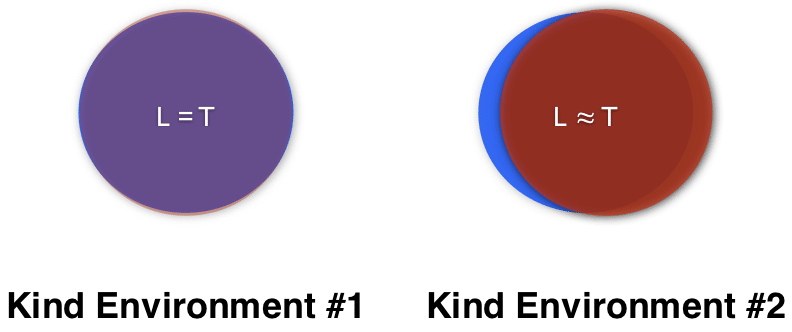
This is because therapy exists in what Robin Hogarth calls ‘wicked’ environment, not a ‘kind’ environment.

Kind Environment
Kind environments are when the feedback loop for the target of learning and the impact of performance are clear. Examples of kind environments include golf, chess, bowling, weightlifting and school homework.
Deliberate practice in the field of psychotherapy is not like weightlifting, where the more you do, the stronger your psychotherapeutic muscles become.
Neither is it like golf, where if you spend more time to improve your putting, you will likely improve your game.
Neither is it like chess. Though it is a game with highly complex strategies, it’s parameters are well-defined; its objective is easy to measure.
In short, weightlifting, golf and chess operate under kind environments.
Wicked Environment
A “Wicked Environment” is where the rules of the context are often unclear, and the feedback loop for the target of learning and the impact on the performance is delayed, inaccurate, or both. Examples of wicked environments include poker, soccer, medicine, and life.
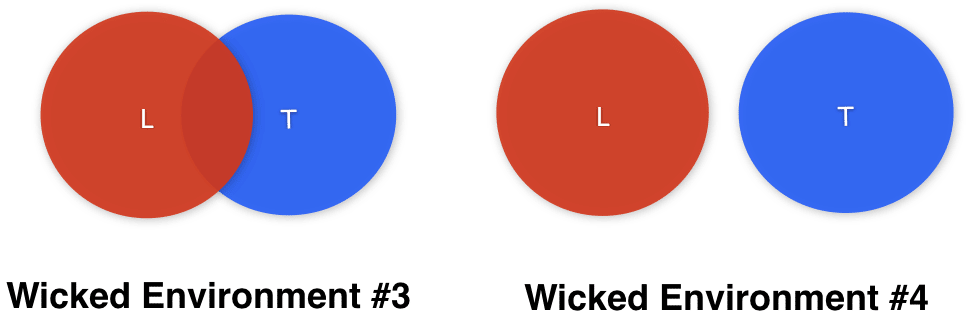
When we practice as if we are in a kind environment, we risk our efforts looking like #4, where our learning efforts does not translate in our targeted naturalistic setting.
If we reshape our efforts and design for learning in a wicked environment, we stand a fighting chance for our professional development efforts to impact our clients’ lives. If continue to think we are in a kind environment, we are likely to make very little progress in the end.
The task of DP is to seek not just what’s right, but what’s right for you i.e., what you need to work on to get at your growth edge. This must also take into account who you are as an individual.
The Science of the Individual, Not the Average
Truth is the conformity of the mind to reality…
Modern man often wants reality to conform to his mind, but truth is the conformity of the mind to reality.
— The Culturist and Ascent
In his book The End of Average, Todd Rose notes that most research studies adopt an averagarianism approach to its investigation. That is, aggregate, then analyse.
First, combine many people together and look for patterns in the group. Then use these group patterns (such as averages and other statistics) to analyse and model individuals.
The problem with this nomothetic approach is that it assumes
Every member of the group is identical and
Every member of the group will remain the same in the future.
This is far from the messy reality. In reality, variation is the norm.
Instead of an aggregate, then analyse approach, Rose proposes we should take a analyse, then aggregate perspective.
Rose explains,
First look for patterns within each individual, then look for ways to combine these individual patterns into collective insights. [emphasis mine]
One way to make sense of this difference between aggregate, then analyse and analyse, then aggregate is to look at an example.
Let’s turn to a specific research on infants.
From the 1930s through the 1980s, scientists who studied infant development wrestle with a puzzling mystery known as the stepping reflex. When a newborn is held upright, she begins moving her legs in an up and down motion that closely resembles walking for a long time. Scientists suggested the stepping reflex pointed to a presence of an inborn walking instinct. But the reason this reflex was so mystifying was that at around two months of age the reflects disappeared. When you hold up an older baby, her legs remain mostly motionless. But then, shortly after the infant begins to walk, the stepping reflex magically returns. What causes this reflects to appear, disappear, then appear again?
Scientists first attempted to solve this mystery with an aggregate, then analyse approach. The researchers examined a large number of infants, calculated the average age of various milestones and their neural development. Scientists soon learned that
…one neural process seemed to correspond with the appearance and disappearance of the stepping reflex: myelination.
Myelination is the essential, developmental process of forming a fatty, insulating layer called the myelin sheath around nerve fibers (axons) in the brain, spinal cord, and peripheral nervous system.
Arriving at this myelination theory using the aggregate, then analyse approach, the scientists proposed that each baby is born with a stepping reflex but as the motor control centre of the brain begins to marinate the reflex vanishes. Then, after the motor control centre of the brain developed further, the baby regained conscious control of the reflex.
The only thing with this explanation, a neural explanation rooted in brain development, was wrong.
This became the standard of care in medical practice, and even served as the basis for diagnosis of neural disorders in the 1960s.
If a baby’s stepping reflex did not disappear on time, physicians and neurologists warned the parents that the child might have some kind of neurological disability.
Then came developmental psychologist Esther Thelen.

Thelen took a different approach.
Between 1979-1984, Esther Thelen conducted a series of ingenious experiments that challenged the medical orthodoxy.
Thelen took an analyse, then aggregate approach.
Thelen studied 40 babies over a period of two years. Every day she took a photo of each baby, examining with their individual physical development. She held them over treadmills and place them in different positions to analyse the individual mechanics of each babies motions. Eventually, she formulated a new hypothesis about what was causing the disappearance of the stepping reflex: chubby thighs.
What?! Chubby thighs?
Thelen showed that when infants are supine (lying on their backs), they perform kicking movements that are identical to upright stepping. Yet kicking didn’t disappear while stepping did. Why?
Simple: physical growth.
Thelen noticed that babies who gained weight at the faster rate tended to lose their stepping reflex the earliest, “simply because their leg muscles were simply not strong enough to lift up their legs.”
But why didn’t the aggregate, then analyse approach not discover this?
Rose notes,
… previous scientists who simply compared average ages to average weights have never discovered anything. The aggregate, then analyse approach disguised each child’s individual pattern of development. Thelen’s analyse then aggregate approach revealed it.4
The scientific community of that time rejected her “chubby thighs” theory. But in a series of experiences between 1982-1984, Thelen proved that her findings reflects reality. Here’s an overview of three studies:
Experiment 1 - Adding Weight: Weights were added to infants’ legs proportional to the weight gain expected between 4 and 6 weeks of age. The infants reduced the number of reflex steps while wearing the weights. This showed that increased leg mass interfered with stepping.
Experiment 2 - The Water Tank (The Breakthrough): Researchers held infants upright in an aquarium filled with water up to their hips. The water reduced the pull of gravity on the legs and made them relatively lighter. When the infants’ feet touched the bottom, the number of steps increased.
Experiment 3 - Tracking Weight Gain: At 4 weeks, infants who gained weight and chubbiness most rapidly performed the fewest steps.
In short, the difference between aggregate, then analyse and analyse, then aggregate can lead us to very different conclusions. When we get closer to the individual, as opposed to the average, this will bring us closer to the truth of reality.
What happens when we ignore the individual of the therapist and focus on the treatment?
Who the treatment provider matters more than the treatment model.
Consider how in the past when studies in psychotherapy used to find that treatment differences (e.g., one approach is more superior than the other). But when researchers re-examined these studies, it turned out that the original investigation treated the treatment provider as an “error variance.” In other words, therapists were removed from the analysis as it was treated as statistical noise.
When the re-analysis was conducted, nesting the “who” of treatment provider into the mix, it washed away treatment differences. Instead, when the statistical analysis matched the reality of various providers into the picture, differences were found between therapists, not between treatment approaches.
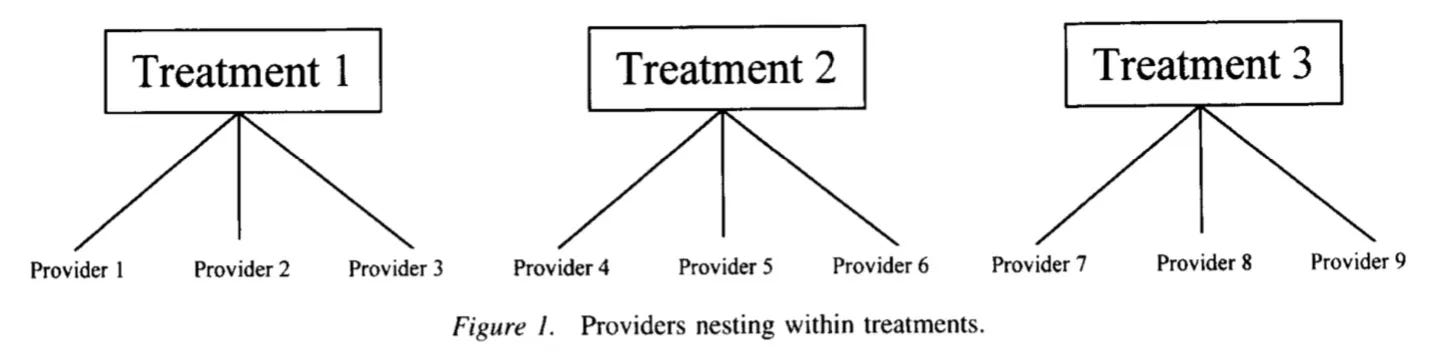
This 2000 paper by Wampold and Serlin highlighted that ignoring therapist effects in psychotherapy outcome studies would falsely inflate the estimates of treatment effects.
I am speculating here, but since this study was published, we have seen a shift in the methodologies employed (i.e., using multi-level modelling), accounting for the hierarchical nature of the therapy (i.e., clients nested within therapists). It has been fairly consistent that therapist effects account for 5-9% of the outcomes in treatment, compared to treatment model differences which account for 0-1% in outcome.
Evidence that suggests “what works for whom” is based on averages. It assumes that clients—and therapists—are homogenous.
We are not an “average” person. No one is.
Our efforts to improve as therapists must also account for the nature and gifts of each individual.
Related:

Can DP Make Things Worse?
Holding the diffferences aside, can DP actually make things worse?
In a 2024 Swedish study, an eight-week RCT manualised DP course found that the DP group experienced a decrease in alliance.
Look at this graph.
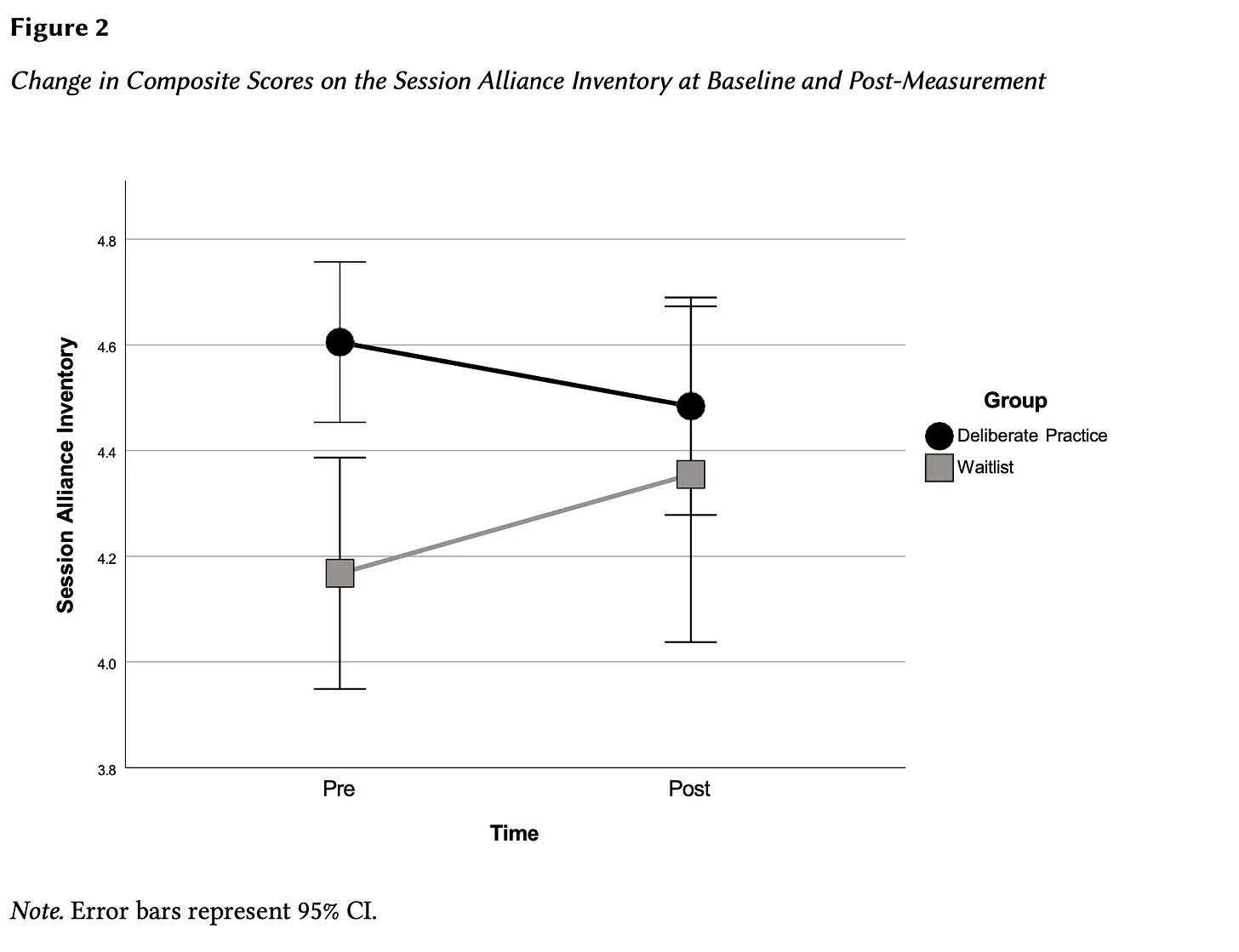
Why is this the case?
Why Engage in DP?
Maybe I’ve been staring at this for too long. Maybe I’m missing something about the merits of “DP” for specific models. I’m prepared to change my mind about this. After all, we are at an early stage of development for DP in our field; the actual published research studies are disproportionate to the amount of books published about the topic.
There’s so much to discover and make progress in.5
I’m not wedded to concepts like DP. I’m not a DP police.
The most important thing is not to lose track of what is the most important thing.
So what’s the most important thing when we are thinking about our development?
Two basic questions we can ask ourselves:
What is it for?
Who is it for?
For me, it is this:
“Are my learning and development efforts actually helping those whom I seek to serve?”
Let’s make sure we keep asking what’s the goal behind the goal, the why behind the why.
To learn more about deliberate practice and its limits:

Depths of Excellence and Ethics. Frontiers Friday #150 ⭕️

People don't care how much you know until they know how much you care.
Notice Board
Thanks to the three Leader Psychology Practice (LPP) teams in the Department of Education, NSW for inviting me over to Sydney. Working with supervisors like you made it a very rewarding and trip. Special thanks to Vashti Casey, Robyn Watkins and Janet Rowe.
Thanks to Australian Educational & Developmental Psychology Association (AEDPA) for hosting a virtual training with me. See you guys once again in early April!
To my fellow Chinese colleagues around the world, I hope you had a good Lunar New Year with your families in the last few weeks.
I’ve just produced another batch of recordings for HomeKit, an audio series to help you get unstuck, just when you need it.
The newly home-brewed, AI-free modules include the topics on i. Comparison, ii. Depression iii. Play.

Daryl Chow Ph.D. is the author of The First Kiss, co-author of Better Results, The Write to Recovery, Creating Impact, and the latest book The Field Guide to Better Results. Plus, the latest book, Crossing Between Worlds.

You might be interested in my other Substack, Full Circles: Field Notes on the Inner and Outer Life. FC is a return to soul and sanity, beyond the hollow promises of self-help tips and tricks.

Unless you become a founder of an approach.
Wampold, B. E., & Imel, Z. E. (2015). The great psychotherapy debate: The evidence for what makes psychotherapy work (2nd ed.). Routledge/Taylor & Francis Group; US.
Webb, C. A., DeRubeis, R. J., & Barber, J. P. (2010). Therapist adherence/competence and treatment outcome: A meta-analytic review. Journal of Consulting and Clinical Psychology, 78(2), 200–211. http://dx.doi.org/10.1037/a0018912
Esther Thelen’s work became foundational to dynamic systems theory of development, popularly called Chaos Theory. Thelen said dynamic systems theory “seeks to understand the overall behavior of a system not by dissecting it into parts, but by asking how and under what circumstances the parts cooperate to produce a whole pattern.”
That said, one of the general efforts we need to make as a field is to reduce the amount of people who fall through the cracks, the unplanned dropouts from treatment, and negative experiences.